Many women with adrenal PMOS (previously called PCOS) have already spent years in the medical system. They have tried the pill, possibly spironolactone, and watched facial or body hair persist regardless. That experience is not a failure of persistence. It reflects a specific biological mismatch between the treatment offered and the subtype of PCOS driving the problem.
For those exploring hair removal for women in Sydney alongside ongoing medical management, understanding that a mismatch is the first step towards a more effective approach.
What is Adrenal PCOS?
PMOS, or Polyendocrine Metabolic Ovarian Syndrome (previously called PCOS or Polycystic Ovary Syndrome), is not a single condition. It presents across several subtypes, and the distinction matters clinically.
The more commonly discussed subtype involves excess ovarian androgen production, often accompanied by elevated LH/FSH ratios, irregular cycles, and visible follicles on ultrasound.
Adrenal PMOS is different. Here, the primary androgen source is the adrenal glands, which produce excess dehydroepiandrosterone sulphate (DHEA-S) rather than ovarian testosterone.
Key distinguishing features of adrenal PMOS include:
- Normal or near-normal LH/FSH ratios
- No cysts visible on ultrasound in many cases
- Elevated DHEA-S on blood testing, sometimes missed if only testosterone is checked
- Delayed or missed diagnosis because it does not fit the classic PMOS presentation
Why Standard Hormonal Treatment Underperforms
The combined oral contraceptive pill works primarily by suppressing ovarian androgen production and increasing SHBG. In adrenal PMOS, ovarian output is not the main driver. The pill addresses a source contributing relatively little while adrenal DHEA-S output continues largely unaffected.
Spironolactone offers more systemic coverage and helps some women meaningfully. However, it does not reverse structural changes that have already occurred.
This is the point most clinical conversations do not reach: even when androgens are brought under control, follicles that have already transitioned from fine vellus hair to coarser terminal hair do not revert.
The hormonal signal that triggered the transition is no longer needed to maintain it. The follicle has undergone structural changes, which are permanent without direct intervention.
| Treatment | Targets Adrenal Androgens | Reverses Transitioned Follicles |
| Combined pill | Partially | No |
| Spironolactone | Partially | No |
| Metformin | Indirectly | No |
| Galvanic electrolysis | Not applicable | Yes, treated follicles permanently |
Why Permanent Follicular Treatment Becomes Necessary
Hormonal management and follicular treatment address two different problems. Hormonal treatment aims to slow the activation of new follicles. Follicular treatment addresses what has already structurally changed.
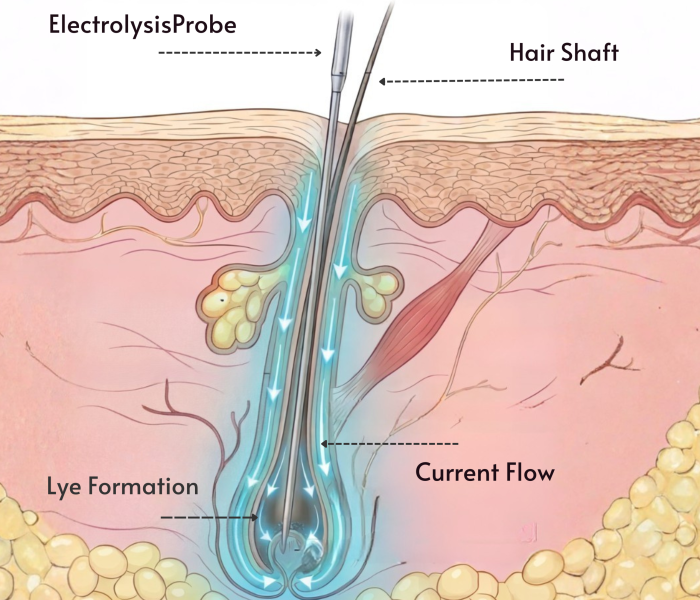
Galvanic electrolysis works by inserting an ultrafine probe into the natural opening of the hair follicle, where a direct current produces a chemical reaction that destroys the stem cells responsible for hair growth.
Once treated, that follicle cannot produce hair again. The process is independent of hormonal changes.
A woman whose DHEA-S remains elevated despite treatment will likely continue activating new follicles over time.
Electrolysis permanently disables each follicle it treats. Consistent sessions progressively reduce overall density, even if the underlying hormonal driver has not been fully resolved.
Why Galvanic Specifically
Galvanic electrolysis uses direct current to produce sodium hydroxide within the follicle. This chemical action is particularly well suited to coarser, deeper terminal hairs that have developed under sustained androgen stimulation.
Additional advantages relevant to this group:
- Does not rely on hair pigment, making it effective for fine or light adrenal-PMOS-driven hair that lasers cannot target
- Works consistently across all skin tones
- Treats the follicle regardless of hormonal status at the time of treatment
Multiple sessions are required because hair grows at different times within its natural growth cycles. Mild tingling or stinging may occur during treatment. Temporary redness afterwards typically resolves within a few hours with appropriate aftercare.
A Practical Note on Medical Coordination
If adrenal PMOS has not been formally confirmed, an endocrinology referral is worth pursuing before or alongside starting electrolysis. Standard panels sometimes test only total testosterone. Asking specifically for DHEA-S gives a clearer picture of adrenal contribution.
Useful markers to discuss with a GP or endocrinologist include:
- DHEA-S
- Free and total testosterone
- SHBG
- LH and FSH
According to Jean Hailes for Women’s Health, PMOS diagnosis requires careful assessment across hormonal, ultrasound, and symptomatic criteria, and subtype distinction is important for guiding appropriate treatment.
Moving Forward
Persistent hair growth despite hormonal treatment is not an anomaly in adrenal PMOS. It is a predictable outcome of addressing the wrong source or failing to reach the follicle level.
Galvanic electrolysis treats what is already there, permanently, one follicle at a time. That is a meaningful distinction for women who have already tried the other options.



